
HELLA Human Elaboration Lifelong Learning Approach
First some wisdom to be meditate on:
In integrating some of Hippocrates thinking in a concentrate version: “A wise man should consider that health is the greatest
of human blessings, and learn how by his own
thought to derive benefit from his illnesses and everyone has a doctor in him or her; we just have to help it in its work. The natural healing force within each one of us is the greatest force in getting well. Our food and walking should be our medicine while Illnesses do not come upon us out of the blue. They are developed from small daily sins against Nature. When enough sins have accumulated, illnesses will suddenly appear”!
Some years later we do have a lot more tools in our biopsychosocial toolbox (of some I describe below), with Hippocrates thinking/poractice in our minds!
Then with specific clinical focuses I have based my work on: “Give a Man a Fish, and You Feed Him for a Day. Teach a Man To Fish, and You Feed Him for a Lifetime” (could be from Lao-Tzu (https://quoteinvestigator.com/2015/08/28/fish/) is the point of departure for my clinical work and below some details – the manual is called “patient as an educated reasonable competent resource and coworker in own rehab”
But “If someone wishes for good health, one must first ask oneself if he is ready to do away with the reasons for his illness. Only then is it possible to help him.” (Hippocrates)
One thing more – a warning, the below is perhaps not what you expect. If so, job what is heavy and go to the pictures and text associated with them – and the start over again, while this is actually (what I believe in the future) a special discipline, not very easy to understand in minutes, not talking about its practice. BUt, as long I can work, I will make priority for those who want to learn with the attempt to further developed basic thinking I have developed ins the footsteps of of George Kelly, who, like me, wanted “followers” be not restricted by specifically his or mine expressions of an idea which is a paradigm which may bring increase direct health promotion or first its rehabilitation at individual´s (ideographic) levels, a win-win process for individuals as well as societies. Pathetic? If you wish, but I think that some well paradigm based thinking needs more than 1, 2 or few promotors – where basic humanistic united give enough energy to bring needed (paradigmatic define) changes into the practices! Is health care inefficient, rigid regulatory system where the patient is lost – at best? | Biopsychosocial Medicine
Synopsis; My clinical approach focuses on
(a) A biopsychosocial medicine toolbox (see the picture below), where I show the multidisciplinary in more details), when it seems main problems are also psychological ones are also preferably physiological (diet, breathing, endorphin-like exercise, etc.) and are important part of the personal guided/supervised tailoring process as well as in the the same ways also for the only seemingly physiological/biological ones, which has a psychological part …
(b) Education manual: “Patient as an educated reasonable competent resource and co-workers in own rehab”, based on my dissertation 1986 represent the manual (more info at other links) and
(c) Examination with psychophysiological stress profiling: psychophysiological measurements are important part in examination/investigation, education/practice (including sometimes integrated biofeedback) and evaluation as well.
(d) Important is the communication with the patient about data based on earlier education (see “b” followed by together workout a intervention plan where the patient take an important part through own actions.
(e) Interventions are mostly based on individual´s (guided when needed) tailoring of the toolbox during education in groups (and personal when needed)
(f) Outcome measures and documentation in terms of IBED (individual Biobehavioral Evidenced based Documentation based on single case design. At best, easily to publish cases without too much work – enabling also clinical communications with colleagues!
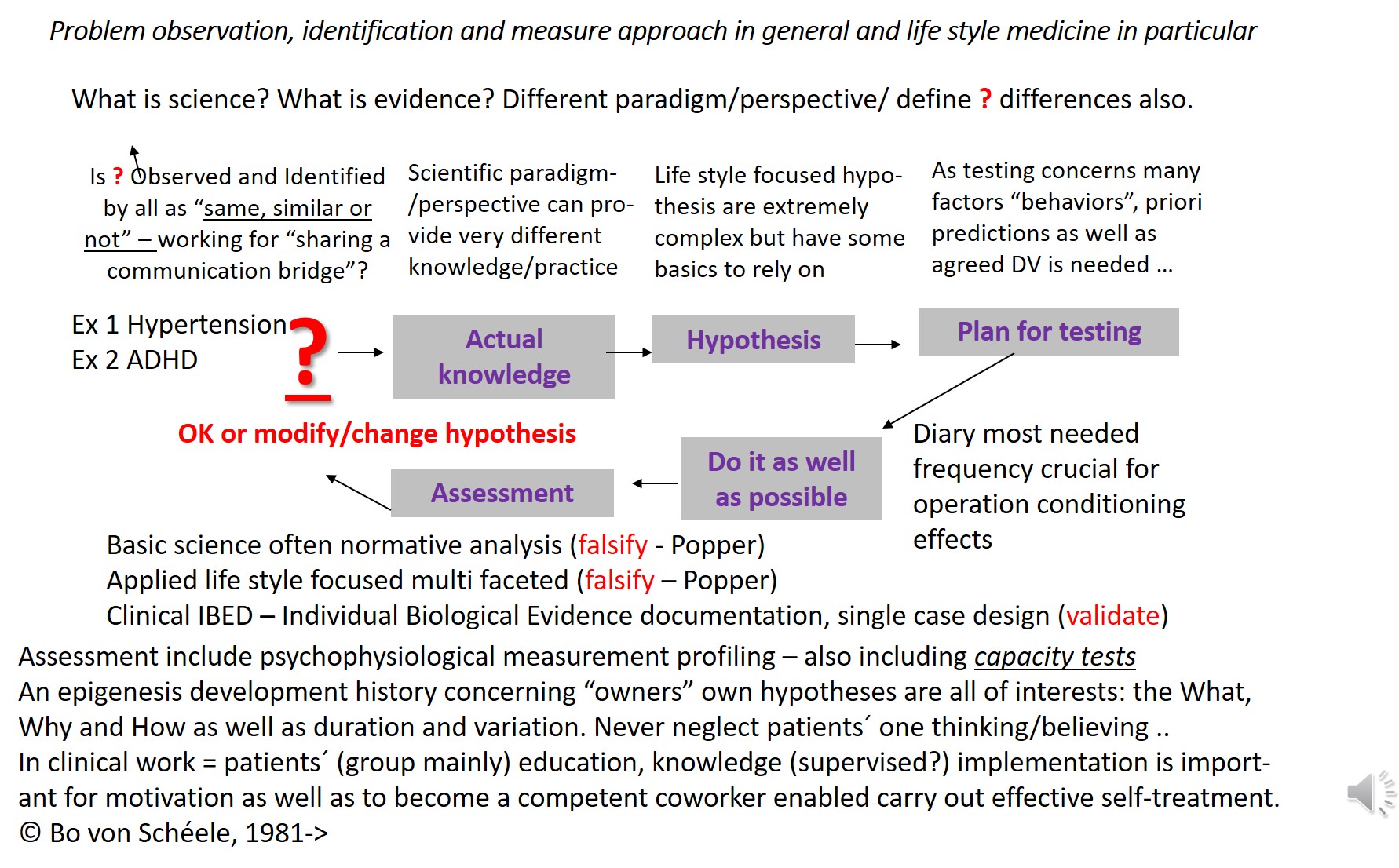
(g) Considering not only scientific paradigm but also methodological considerations see e.g.Evidenced based falsification of data or validation of the individual patient in front of us? | Biopsychosocial Medicine
(h) Enabling clinical education (see more just below)
The educational process (where integrated psychophysiological behavioral medicine play a critical role*) suggested in groups enable not only reasonable understanding, active co-working (including self-activities) but also increased motivation (* they see – observe and understand – what they do and do what they see) as well as develop a biopsychosocial effective life style habit enabling sustained or increased health development. Too much and too expensive and too complex? Maybe, but this is not my experiences. Critical is to invite interested clinicians to a “laying-puzzles workshop series” enabling working full time, have family while learning the above … – this is what I try to do at www.ipbm.se (will be updated in Swedish).
Below I do not discuss eastern medicine (and what I regard as very important to integrate) but refer to Eastern and western medicine – can they both meet in win-win using an integrating psychophysiological platform? | Cultural Medicine Why? While I do think we have much to learn, especially from Qui Kung, about thousands of years experiences of health promotion and prevention of diseases due to self-care activities/behaviors. Representing a tradition we may respect in our mainly pharmacological based western medicine – something we can learn very much from. Working with psychophysiological stress medicine, it has been easy to learn and modify for Swedish use – an attitude perhaps not many shares with me. Hmmmm what about evidenced based research? Hmmm my argument is (for some perhaps too) provocating (not my intention) but see e.g. Are common reductionistic evidenced based clinical research meaningless, at best? | Biopsychosocial Medicine for my proposal (quite out of main stream I am used with since 40 years .. while still continue with the best intensions out of my paradigm)
NB the below is very incomplete so far, just add it to refer to those I think it can give some idea of my work since 1986, not really anything published after my dissertation, but my thesis is over the years refined during clinical work with many different patient populations.
Below is (at last) a very first very small step to document my work during the years… more will come when my health is better …
The reason for not publishing is not only lack of time (many patients in priority but also money to write) but also that I each day improve my work so all will be old next morning. Since long, I focus on writing on websites, where I can update continuously …
Draft:
Much is discussed about critical education, e.g. Thales (Summarized of the paradigm used by Bo von Schéele | Biopsychosocial Medicine – NB in Swedish = Vetenskap | Stressmedicinsk Centrum (stressmedcenter.com) but not much about an evolutionary point of departure of human development including Triune Brain https://en.wikipedia.org/wiki/Triune_brain as well as Dual-coding theory https://en.wikipedia.org/wiki/Dual-) coding_theory#:~:text=According%20to%20Paivio%2C%20there%20are,is%20used%20to%20represent%20information.&text=Both%20visual%20and%20verbal%20codes%20can%20be%20used%20when%20recalling%20information
I also work with a quite new way to try to in practice based my understanding on Quantum Biology (www.quantummedicine.website) concretized in a very special psychophysiological approach – first with myself as the subject, before I (by “Hippocrates” reason) start with some clinical cases …
NB I do not discuss details below, and I only have the links above as indication of (a) what (I regard) we need to consider about the evolution of human and especially human brain as a gradually extension over million of years – as Zimbardo said – “a house jerk”. Reptilian, Limbic Mammalian (spatial) were human brain (verbal) is the last step – so far – and we have to be aware and consider this impossible possibility – what we are “equipped” with! Hard? But, that is what we have to deal with. The good news is that we do could survived thanks to our ability to process incomplete information, which is not the case for (especially old) computers.
So, in spite of lack of knowledge about how spatial and verbal systems interplay as well as with more basic reptilian brain (in humans), we do need to try to incorporate it while it is apparently what is the foundation of human mental information processing. See more at How to deal with not absolut knowledge – which no one of us have access to | Biopsychosocial Medicine + http://culturalmedicine.se/health-in-complex-world/toward-development-of-a-guide-facilitating-knowledge-and-practice-based-use-of-human-limbic-systems-information-processing-in-general-and-health-care-services-in-particular/cutural-evolution-of-human-brain-based-on-our-very-much-modified-interacting-mammalian-and-reptial-brains/ + http://culturalmedicine.se/health-in-complex-world/toward-development-of-a-guide-facilitating-knowledge-and-practice-based-use-of-human-limbic-systems-information-processing-in-general-and-health-care-services-in-particular/ + http://biopsychosocialmedicine.com/paradigm/summarized-of-the-paradigm-used-by-bo-von-scheele/ + .
Relying on the work of George Kelly, who was much influenced by John Dewey https://en.wikipedia.org/wiki/George_Kelly_(psychologist) and further develop his “man as a scientist”-metaphor, I have used in my pedagogical clinical work all years, an approach I now call HELLA.
By focusing on “?” independent of what is the present “?-target” – also used it as folk high school teacher – I have found it promising in patient group education using a manual based on my dissertation 1986 “COOL, Chief of One Own´s Life” = “Co-Decision” in Life, (the Swedish “Medbestämmande livet” can not really be translated while a special part of our cultural development) in the clinical expression “patient as a reasonable well educated resource and coworker in own rehab”, that is a biopsychosocial medicine toolbox where patient are tailoring there own tools.
Here is the HELLA included to be used when an individual have a “?” or are encourage to become asking a “?”.
Below I only discussed HELLA strategy briefly. Later on, writing in more detail.
But first the toolbox COOL:
(COOL, the Chief of One´s Own life – was the title in my dissertation 1986)
Since 1983, I have used the biopsychosocial toolbox as a manual in various trainings not only clinically with patient groups – and then further developed it over the years. The starting point is that the user should reasonably understand the tools (why they can be useful given they are tailored by each user in cooperation with supervisors. The measurement system of psychophysiology constitutes a “third party” (where possible) in tailoring. Importantly, the user himself sees his possibilities and thus feels motivated from there to implement the self-activity program that is proposed – based on explanations but has understood (!) in the psychophysiological investigation that forms the starting point (see more at e.g. To SEE or not to SEE makes a diference | Skills before pills

The HELLA strategy 1:
1. The WHAT – are the problem picture and its different (biopsychosocial-cultural?) consequences? Patterns and relationships? Often, just reviewing and processing “what” is not enough, but moving on to solutions … thus, go back to the “what” during the problem-solving process from time to time …
2. The WHY – “factors” (often several, which one may not “see at the first moment”) have arisen and develop “1” – can these factors interact in a synergistic way?
3. The HOW – can we find ways to solve “1 and 2”? I suggest you use the approach below…
The HELLA strategy 2:
Comments:
First, patients´ group education was “normally” 2 hours each week in 6-10 weeks. Goal was to result in a practical knowledge base where they have started up tailoring of their tools. Hopefully, also influence there general health development due to more life style health promoting behaviors (based on our actual knowledge we (supervisors) have learned/used (ourselves) etc.
Then, important following Kelly´s approach (as I have used it in this case) try to start from the person´s knowledge position and base changing processes on dialogue, enabling the person to internalized changes. Really feeling being an active (not passive) part of their own development
What patient population can be addressed?
Most lifestyle related, in medicine especially hypertension is the easiest population to start with (given you do have my work program to start up before further develop and tailor for your own ambitions/ideas/…
In psychology. I regard ADHD as the most important to address! see e.g. www.adhdfonden.se ..
I have worked during the years with many “difficult” patients, severe PTSD (As torture victims), stress prevention at work places (a special program called “visit and test at different stations -workshops”) and with education, where patient education, which I find very inspiring!
More is coming ..
Furthermore, …
More is to come .. I hope